Lymphoproliferative disorders & renal disease
All of them can affect kidneys: Hodgkins/non- hodgkins, post immunosuppressive (EBV etc) CLL, Waldenstroms etc
Almost all patterns of injury can occur. The unique factor is that a monoclonal protein may light up on the IF. Hence the benefit of doing Kappa and Lamda and CD3,CD20 when suspicious.
Renal involvement
- Direct infiltration
- Glom/tubulointerstitial/vascular lesions due to monocloncal protein
- Glom lesions due to cytokines
- Paraneoplastic (amyloid, acid-base)
- Intravascular invasion – gloms can become occluded by the atpypical lymphoid cells- A wee bit like tx glomerulitis – AKI, fever, weight loss
- Indirect: nephrocalcinosis, tumour lysis, hyperviscosity syn, DIC, TMA, TIN, Drugs
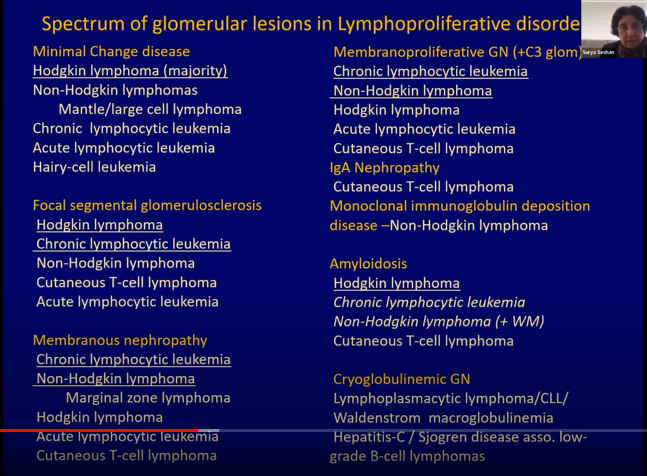
Glomerular lesions:
Hodgkin: MCD, FSGS, AA Amyloid
Non-Hodgkin: T cell Cytoine med podocytopathy, MCD, FSGS
B cell with monocolonal gammopathy:
- Cryoglobulins – granular/tubule-fibrillar
- Non cryos: granular/tubule-fibrillar/crystalline
- Other: AL amyloid, cast nephropathy, light chain tubulopathy
CLL can make a gammopathy and has a tissue phase
Waldenstroms is the lymphoma that pumps out IgM. 30-40% of IgM kappa can be cryoglobulins, so test for same if you find it on bx.
Suss
- Older age group
- History of MGUS/lymphoma – can be historical
- Any abnormal pattern on bx, anything weird about an interstitial infiltrate ( like monomorphic, nesting and clumping a bit)
- Get a CD3 (t-cell marker) CD20 (B- cell marker) and Kappa and lamda LC stains
Notes
Treat the underlying cause to improve/cure kidney disease
Kidney recurrence can herald lymphoproliferative recurrence, or be a first presentation/predate
Wide age range of patients but many series report older predominance (>60) ?male
Duration between lymphoma and renal disease can be >10 years
In glomerular lesions, tend to be CKD picture, nephrotic syndrome common, about 20% haematuria, gammopathy common, 60% perhaps
In parenchymal lesions, no NS obviously, only about 13% have a gammopathy but mass on imaging sometimes
LN and BM biopsy useful adjunctive tests
Primary extra nodal lymphoma in a kidney is a thing, but extremely rare
Make friends with a haematologist