- Membranous like glomerulopathy with masked IgG Kappa deposits
- MISC
- NELL 1
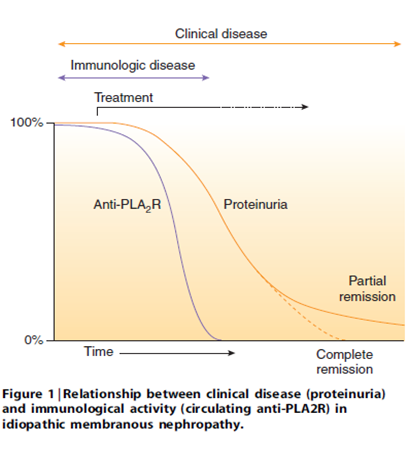
- PLA2r
- Membranous like glomerulopathy with masked IGG kappa despots (MGMID) AKA serum amyloid P associated glomerulopathy
dont need spikes on bx, subepithelial deposits on the EM will do
Membranous like glomerulopathy with masked IgG Kappa deposits
Light microscopy = classic MN, 25% proliferative changes. Routine Negative IF. But on EM you can see the sub epithelial, and mesangial changes.
Paraffin IF – opens up epitopes for ab to bind. Lights up the masked IgGk deposits.
Laser capture microdissection suggests serum amyloid P might be an antigenic target
Young females, preserved renal function, nephrotic range proteinuria, 55% positive ANA, 2% met SLE criteria
Orphan disease - treatment unclear, 44% CKD/ESKD.
Can recur in transplant.
Probably an autoimmune disease rather than paraprotein disease.
MISC
Idiopathic membranous can antigen switch (e.g. IgG1 early and IgG4 later in disease)
NELL 1
NELL 1 in primary membranous
~ 5% +
10 years older than primary membranous
33% had a history of malignancy
Folic acid association?
Mercury containing compounds association?! (e.g. whitening cream)
PLA2r
Membranous like glomerulopathy with masked IGG kappa despots (MGMID) AKA serum amyloid P associated glomerulopathy
- Requires Paraffin IF to make diagnosis
- Rare, 41 cases, IF neg, paraffin IF – Strong IgG -Kappa staining
- Young (mean age 26), white, vague autoimmune. Tends not have NS. no underlying neoplasia. 25/26 neg electrophoresis. (Larsen, KI reports 2016)
- Laser captures microdissection identified serum amyloid P (using mass spec). Can confirm diagnosis by staining with serum amyloid P.